Instructor's key for self-assessment slides (Instructor's introduction)
THIS PAGE IS FOR INSTRUCTORS.
Here are comments intended to help an instructor guide students during their examination of each slide, with extended notes for specimens that present special difficulties.
The page for students is Instructions for examining self-assessment slides
If you are a student learning histology, please realize that the power of this exercise relies on NOT having easy access to slide identification, so that you can gain the experience of really knowing what you are seeing, with well-founded confidence that does not depend on interpretation by outside experts. Please return to Hints for individual slides.
SLIDE INDEX
Slides for CRR slidebox
Slides for ERG slidebox
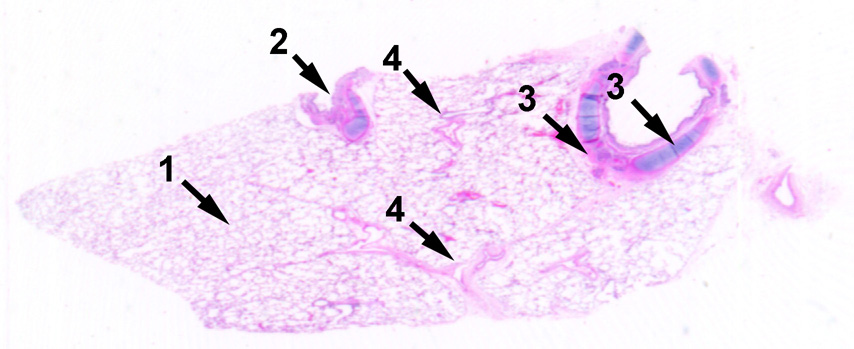
Slide CRR 01. Rather obviously, this specimen belongs to lung, with its texture consisting mostly of alveoli. Bronchi with cartilage, as well as smaller bronchioles, both lined by columnar/cuboidal epithelium, should be distinguished from veins and arteries lined by simple squamous endothelium. A small bronchial gland might be found.
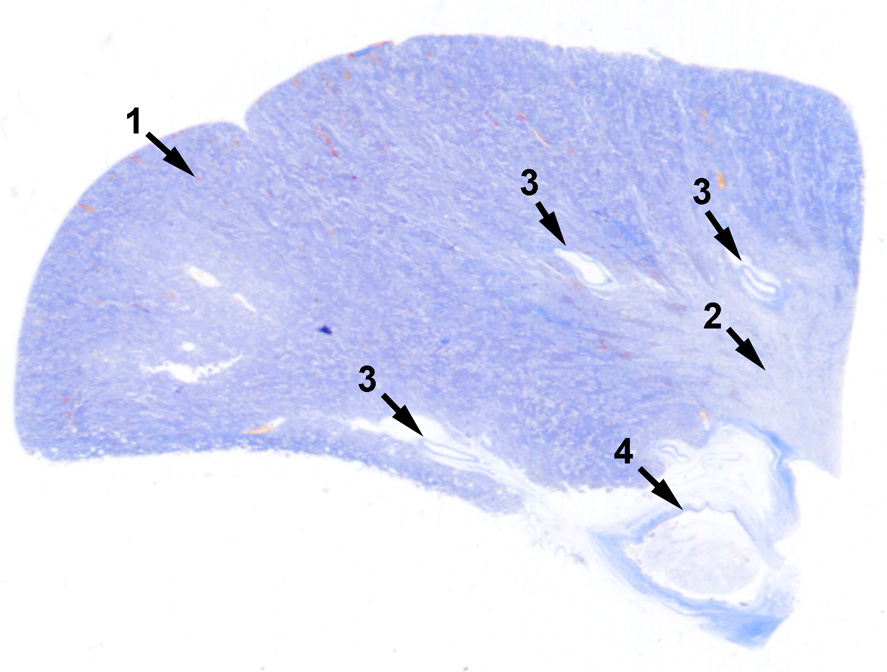
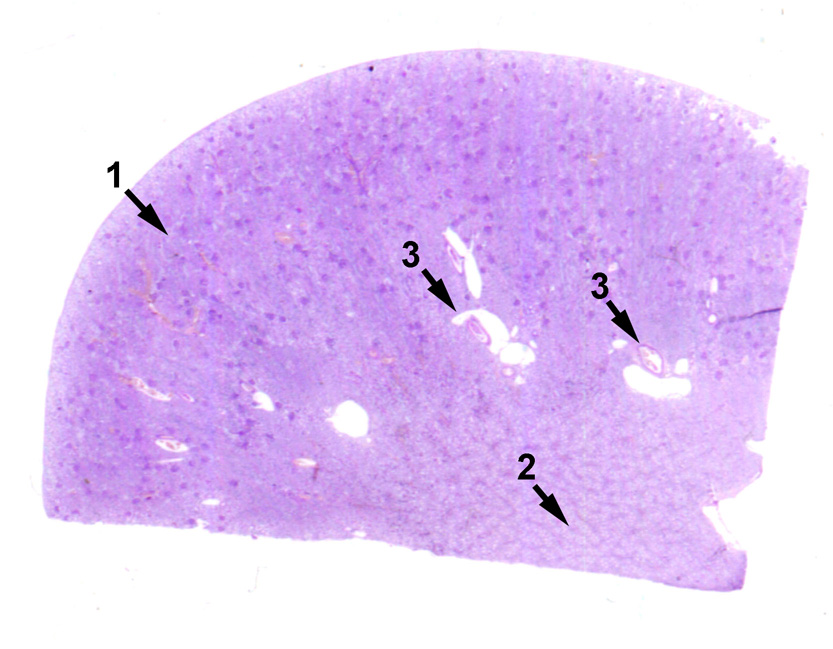
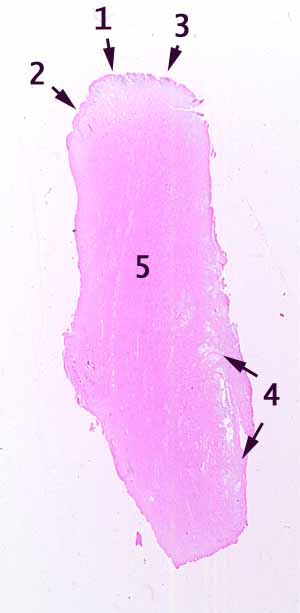
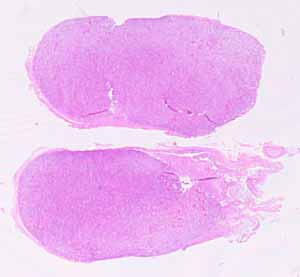
Slide CRR 02. Collagen is colored blue rather than pink on this trichrome-stained slide. Cut surfaces define two relatively flat sides of the specimen. The remaining rounded, uncut surface suggests the size and shape of the source organ. Not too far inward from the natural surface are many renal glomeruli, definitively establishing this specimen as kidney.
The trichrome stain makes it easy to appreciate the existence of collagen in the stroma surrounding renal tubules and glomeruli. Cortex and medulla can be distinguished. The region labelled 4 might need some interpretation to understand as the tip of a renal papilla, belonging to a lobe that is otherwise out of the plane of section.
Slide CRR 03. This specimen has been cut on two sides, while the other two sides display natural surfaces. Neither of the natural surfaces has characteristic features of a mucosa, which should exclude many conceivable sources. Identification depends on recognizing that this specimen is mostly muscle; furthermore it is neither smooth muscle (whose characteristic fibers would be thinner) nor skeletal muscle (fibers much thicker).
The source organ here is heart, so it might be fairly obvious to students looking in a slidebox containing mostly specimens from Cardiovascular, Respiratory, and Renal systems. The epicardial surface here is fairly smooth, while the endocardial surface displays some folds or irregularities.
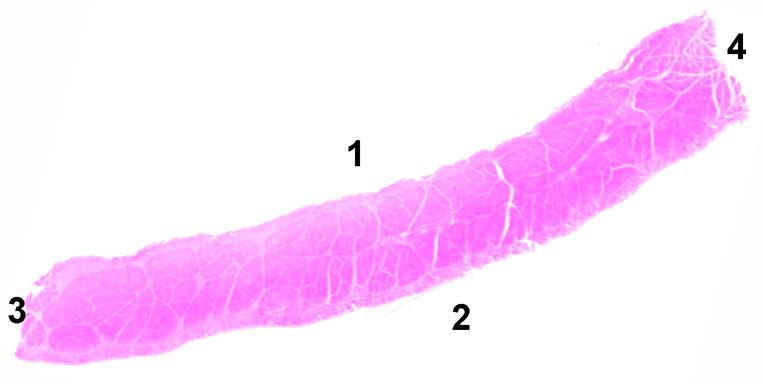
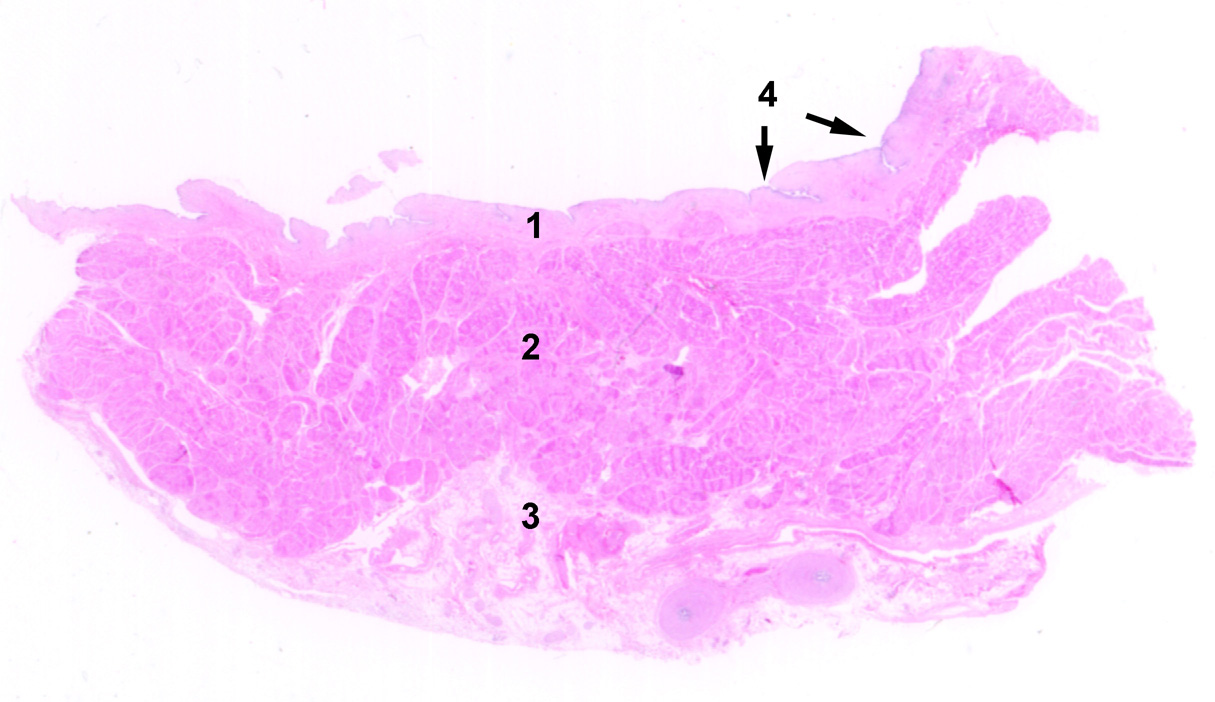
Slide CRR 04. The two ends of this specimen (3 and 4) are cut, while the two sides (1 and 2) are natural surfaces. Its bulk consists of uniformly-sized eosinophilic units, which should be recognizable as skeletal muscle fibers.
What makes this specimen peculiar is that all of these fibers are cut in cross section, not longitudinally along the length of the specimen. Thus the shape of this muscle must be a flat sheet (rather than, say, a tapered cylinder). Knowledge of gross anatomy is essential here, to suss out what muscle could possibly be consistent with these observations: The source for this specimen is diaphragm.
(This specimen also displays some nerves. Any student who notices and recognizes a muscle spindle on this specimen deserves a gold star.) .
Slide CRR 05. The source of this specimen should be fairly obvious. Its identification as kidney may be readily confirmed by observing renal glomeruli in cortex. This specimen provides excellent opportunity to examine many aspects of kidney, including distributing arteries and, in medulla, vasa recta.
Slide CRR 06. Flat, cut surfaces define two sides of this specimen. The remaining rounded, uncut surface suggests the size and shape of the source organ. Like slide CRR 05, the conspicuous presence of many renal glomeruli easily confirms kidney as the source. This specimen is stained by PAS stain, permitting visualization of glomerular filtration membranes.
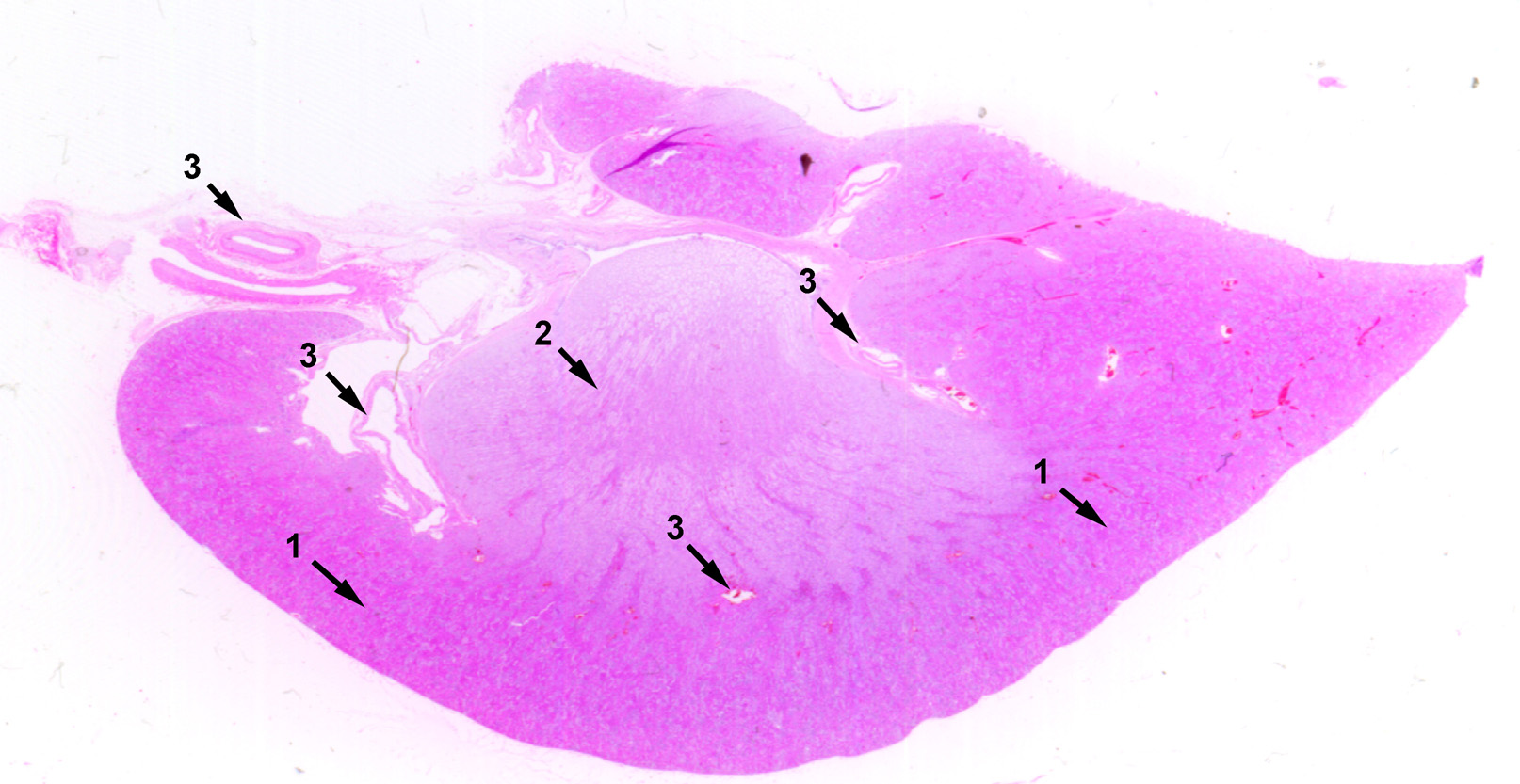
Slide CRR 07. The most conspicuous feature of this specimen is a relatively thick layer of smooth muscle (2 in this image). Unfortunately, the apparent mucosal layer (1) lacks most of its epithelial surface, lost to post mortem change. Remaining shreds of epithelium (4, which help establish that this is indeed a mucosa), are too sketchy for confident identification, but they do suggest a stratified epithelium. Remaining features do not correspond neatly with any part of the GI tract.
The key for identifying the source of this specimen is a site in the deeper tissue. Near the bottom right of the image here, the plane of section intersects twice with a single curved tubule, creating a pair of oval profiles. This tubule has a muscular wall that that is remarkably thick for such a small tubule. It is also lined by a distinctive epithelium. Those features identify this tubule as vas deferens. Gross anatomical consideration of the vas' route through the body establishes that the underlying tissue must belong to bladder wall.
Slide CRR 08. A flat, cut surface defines one side of this specimen. The remaining rounded, uncut surface suggests the size and shape of the source organ. The acidophilic boundary layer (1) is collagen of the organ's capsule, Similarly stained patches within the body of the organ represent extensions from this capsule (trabeculae, 5).
Only one encapsulated organ with this size and shape has the inner texture seen here. This organ's parenchyma includes many small patches (3) that are packed with lymphocytes. Their relatively uniform shape suggests that these are cylindrical in shape rather than spherical. The background texture (e.g., 4), between these lymphoid patches, also consists of numerous lymphocytes but mixed in among red blood cells. Only one lymphoid organ -- spleen -- displays all of these features.
Slide CRR 09. Note the actual size of this specimen on the slide. It consists of two small lumps surrounded by connective tissue. Each of the lumps is packed with lymphocytes and includes small patches (1) where the lymphocytes comprise a paler area surrounded by more densely-packed cells. The central region of each lump (2) has a different texture, still packed with lymphocytes. This is a pair of lymph nodes, without enough context to determine what part of the body they came from.
Slide ERG 01. The distinct layering of mucosa, submucosa, and muscularis should immediately suggest the digestive tract, while the characteristic short crypts together with the absence of villi are sufficient to identify this as colon.
Slide ERG 02. The appearance of this specimen is somewhat confusing, for two separate reasons:
- First, a rather long tissue sample has been folded so that the plane of section intersects the tissue differently in different areas. Follow the dotted line to continue along the length of the specimen.
- Second, most of the surface epithelium has been lost, leaving behind "naked" lamina propria. (This is a fairly typical post-mortem change.) Nevertheless, some characteristic epithelium can still be easily found in protected sites deep in the mucosa. The shape of the missing epithelium may be reconstructed by using your mind's eye to cover the naked lamina propria with simple columnar epithelium.
In the region indicated by 2, the mucosa offers a conventional cross-sectional perspective, so this is a good place to begin. In this region, typical GI tract layers of mucosa, submucosa, and two-layered muscularis should be plainly visible, even though (as noted above) the lamina propria often appears "naked" because of missing epithelium.
In the region indicated by 1, the plane of section is somewhat tangential, which is informative in a slightly different way.
Overall, the shape of the mucosa (with extensions representing plicae), together with the epithelium remaining in crypts deep in the mucosa, should suggest that the source is somewhere along the small intestine.
Slide ERG 03. This has often been a difficult slide for students to identify. One difficulty is that much of the mucosal epithelium has been lost to post-mortem change. But its "trickiest" aspect seems to be that the actual source simply does not even occur to many students.
Once "cervix" enters into consideration, the online hints for this slide, notably the epithelial difference between areas 2 and 3 (even though some epithelium is missinng in between) should be sufficient to guide students to the correct identification -- smooth muscle (5) associated with a mucosal transition from stratified squamous epithelium of the external os to columnar epithelium along the os. Uterine glands may be seen at 4.
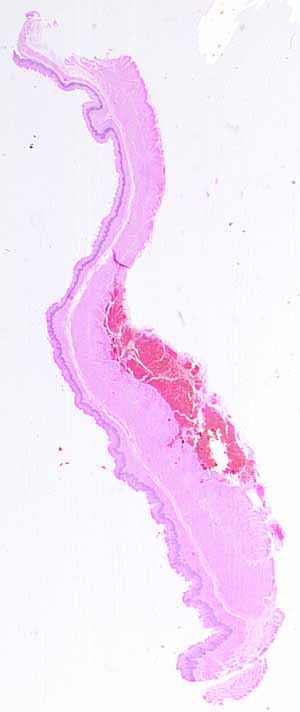
Slide ERG 04. The conspicuous red mass of spilled blood on this slide is just a distraction. Apart from that, the clear layering of mucosa, submucosa, and muscularis should immediately suggest the digestive tract.
However, as I sit here at home writing this page, without access to the actual slides, I am not entirely certain which region of the tract is represented here.
I haven't looked at these slides since I retired over a decade ago, and in this particular case neither the thumbnail image nor the online hints provide sufficient detail for confident recognition. Nevertheless, I believe that this slide demonstrates the importance of inspecting inspect an entire specimen. Failing to so here will yield an identification that is partially correct but incomplete.
Examining the entire length of the mucosa should locate a transitional region where one type of epithelium ends and another begins; thus this specimen includes a transition between two distinct regions. If so, I suspect that this specimen spans the junction of esophagus with cardiac stomach.
Slide ERG 05. The clear layering of mucosa, submucosa, and muscularis should immediately suggest the digestive tract, while the thick mucosa with distinctive glandular texture belongs nowhere else but stomach.
Slide ERG 06. Only one organ in the body is built from so much smooth muscle that its full thickness cannot be included on a typical slide. Such a thick muscular layer (myometrium) together with a distinctive mucosal layer (endometrium) should readily indicate "uterus." As with slide CRR 03, the actual source for this specimen might not readily occur to those students whose bodies do not possess this organ.
Slide ERG 07. This specimen has been cut on two sides, while the other two sides display natural surfaces. Neither of the natural surfaces has characteristic features of a mucosa. Identification depends on recognizing that this specimen is mostly muscle; furthermore it is neither smooth muscle (whose characteristic fibers would be thinner) nor skeletal muscle (fibers much thicker).
The source organ here is heart. This might surprise any students who were expecting only specimens from Endocrine, Reproductive, and Gastrointestinal systems in this slidebox.
The epicardial surface here is fairly smooth, while the endocardial surface displays some folds or irregularities.
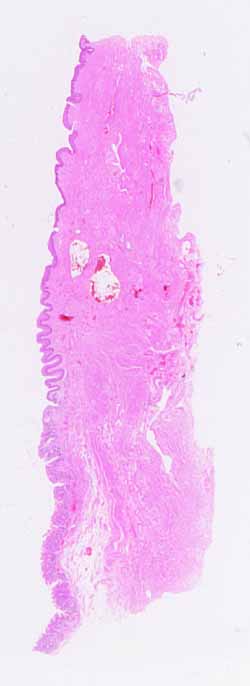
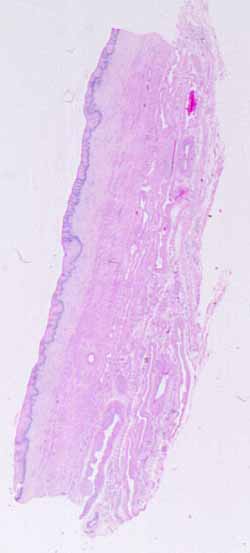
Slide ERG 08. This specimen has been cut at both ends, as well as through deeper (abluminal) tissues along the right side. Also, rather obviously, this specimen has an epithelial surface.
Even with the unaided eye, it should apparent that both the mucosa and the deeper tissues display substantial variation along the length of the tissue sample. Thus this slide should reward especially thorough examination.
Toward the upper end is stratified squamous epithelium. From top downward, this epithelium transitions gradually from keratinized to non-keratinized. (Stratum granulosum is the most reliable indicator of keratinization; the outermost layers of both keratinized and non-keratinized layers can be tricky to distinguish with confidence.)
Mucosa on the lower portion of this specimen displays simple columnar epithelium, with a configuration resembling colon. Unfortunately, epithelial cells displaying the transition from stratified squamous to simple columnar have been lost on this specimen due to post-mortem change.
Variation in underlying tissue layers, both connective tissue and muscle, correlates nicely with the epithelial transitions. Connective tissue resembling dermis of skin can be seen beneath the stratified squamous epithelium in the upper region of this specimen. Connective tissues resembling lamina propria and submucosa can be seen toward the bottom of this specimen, beneath the simple columnar epithelium. Muscularis mucosae can be found where the mucosa is cut at the bottom of this specimen; this layer can be followed upward until it stops near the transition from simple columnar to stratified epithelium. Similarly, loose connective of submucosa at the bottom of the specimen gives way to more densely fibrous connective tissue toward the top.
The anal canal includes just such a transition from colon to skin.
Slide ERG 09. The most conspicuous feature of this specimen is a relatively thick layer of smooth muscle (2). Unfortunately, the apparent mucosal layer (1) lacks most of its epithelial surface, lost to post-mortem change. Remaining shreds of epithelium (4), which help establish that this is indeed a mucosa, are too sketchy for confident identification, but they do suggest a stratified epithelium. Remaining features do not correspond neatly with any part of the GI tract.
The key for identifying the source of this specimen is a site in the deeper tissue, right of center near the bottom of the image here, where the plane of section intersects twice with a single curved tubule, creating a pair of oval profiles. This tubule has a muscular wall that is remarkably thick for the tubule's small size. It is also lined by a distinctive epithelium. Those features identify this tubule as vas deferens. Gross anatomical consideration of the vas' route through the body establish that the associated smooth muscle and mucosa must belong to bladder wall.
Slide ERG 10. The unaided eye reveals this specimen to be entire (with uncut surface all the way around), displaying a very distinctive shape. This alone is enough for recognition of adrenal gland. The structure of cortex and medulla also create an appearance very different from that any other gland.
Note the peculiar and characteristic bands of smooth muscle in the medullary veins. Also note that the connective tissue around this specimen includes brown fat, with each cell having many small fat droplets rather than a single large droplet. (A gold star for any student who notices the brown fat before reading the hints.)
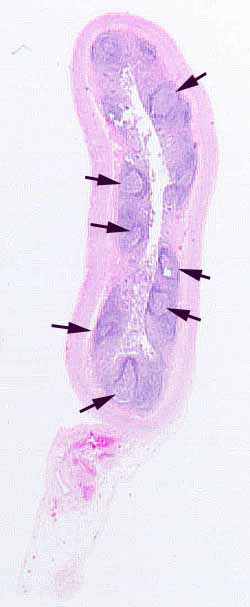
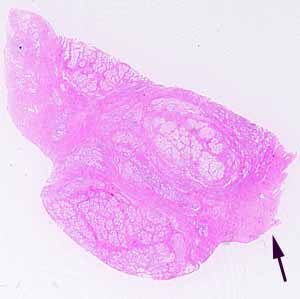
Slide ERG 11. The specimen is entire (with an uncut surface all the way around). Its size together with the numerous lymph nodules in the mucosa (arrowheads) are diagnostic for appendix. Although most of mucosal epithelium is missing due to post-mortem deterioration, it remains visible deep in a few crypts.
Slide ERG 12. This specimen obviously comes from a layered organ, one whose non-keratinized, stratified squamous epithelium might initially suggest esophagus. However, sesophagus can be ruled out by the absence of clearly defined layers. The wall of this organ does not display distinct submucosa, nor distinct layers of circular and longitudinal muscle.
Positive observations include:
- Many small bundles of smooth muscle thoroughly interwoven with connective tissue throughout the wall of this organ;
- Very extensive vasculature, including noticeable veins quite close to the surface (unlike skin);
- Extensive innervation, with lots of conspicuous nerves (several slides from this specimen also include a parasympathetic ganglion).
- Very pale cytoplasm (appearing "empty") in cells of the stratified epithelium.
These observations are all characteristic of vagina.
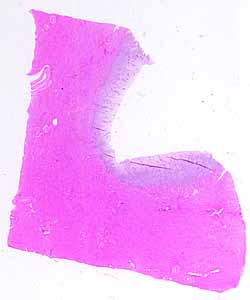
Slide ERG 13. Appearance to unaided eye suggests that this a solid organ subdivided into lobules. Low-power examination reveals ducts; hence this an exocrine gland.
While preparing this page, I don't have access to the actual slides. I am having trouble reconciling the online hints with what I can see in the low-resolution image here. There might be an error in the hints (I hope not) or my memory of what these slides should be might be slipping.
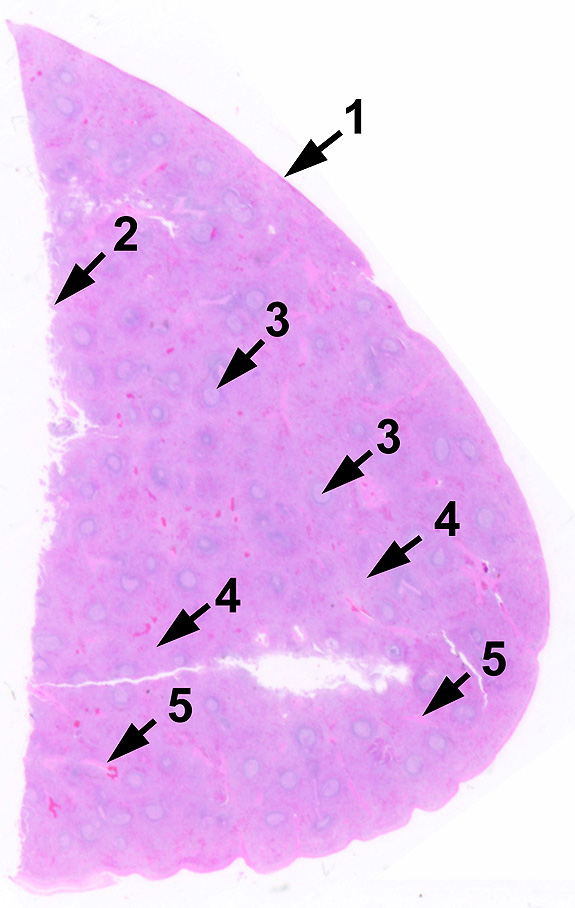
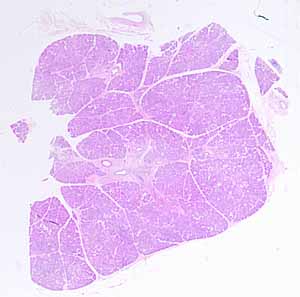
Slide ERG 14. Appearance to unaided eye suggests a solid organ subdivided into lobules. Low-power examination reveals ducts, hence this an exocrine gland.
This particular gland can be distinguished from any other exocrine gland by the peculiar presence of pancreatic islets. These may not be obvious, but once noticed the islets can be seen to have cellular arrangement and staining quality different from the exocrine acini.
Another characteristic, albeit inconspicuous, detail of pancreas is the occasional appearance of centroacinar cells. These are only seen when the plane of section passes through the center of an acinus. Centroacinar cells can be distinguished from secretory acinar cells not only by their central location in the acini but also by their prominent oval nuclei. To be sure, this detail is but one among many curious histological trivia. But practiced skill at noticing such minute details can be key to accurate histopathologic diagnosis.
This is a nice specimen for examining additional glandular details. Interlobular ducts are readily noticeable, surrounded by conspicuous connective tissue. The largest have stratified epithelium. Intralobular ducts are more numerous but more care is needed to find them among the acini that comprise the bulk of this specimen. Cytoplasm of cells forming the epithelium of these small ducts is not conspicuously polarized, in contrast to cytoplasm of the far-more-numerous secretory cells.
Slide ERG 15. This specimen displays cut edges on all sides, so it must have come from within solid tissue.
The small patch of skeletal muscle should not be overlooked. It establishes that this tissue does not come from any organ within any of the body cavities.
Other prominent features include extensive fibrous stroma and fairly abundant fat. Clusters of ducts are also evident. The key observation here is that these ducts are not associated with any noticeable secretory tissue. Hence this appears to be an inactive gland.
All together, these features should suggest breast tissue. As with slides ERG 06 and ERG 12, the actual source for this specimen might not readily occur to those students whose bodies do not feature this tissue.
Slide ERG 16. The edges of this specimen are cut all the way around, so it must have come from within a solid organ tissue. A bit of skeletal muscle (arrow) assures that this specimen did not come from within the peritoneal cavity.
Characteristic features include glandular tissue with thick fibro-muscular stroma. The appearance of irregular tubules lined by convoluted, columnar epithelium is typical of only one gland. The presence of smooth muscle woven in among the stromal collagen is also characteristic of this gland. Both of these features together identify this as prostate.
Slide ERG 17. The innumerable, closely-packed small nuclei throughout this specimen should be recognized as lymphocytes. These cells are clustered into many patches, with relatively pale cells toward their center partially surrounded by darker areas of more-densely-packed cells. These observations should suggest well-organized lymphoid tissue rather than inflammation.
The presence of fairly dense connective tissue on the deeper, cut surface, together with stratified squamous epithelium near the uncut surface, together with deep crevices or crypts that approach all the deep lymph nodules, identify this as tonsil.
Slide ERG 18. While preparing this page, I don't have access to the actual slides. And I can't see any distinctive features in this low-mag image. Unfortunately, the only hint on the hints page is that "this specimen is too easy for hints."
I don't remember with certainty what the source for this specimen really is, but since nothing else looks like thyroid, this organ certainly fits the description of "too easy for hints." What I can see might be consistent with "thyroid," and I recall (from more than a decade ago) that there might be a thyroid specimen in this slidebox.
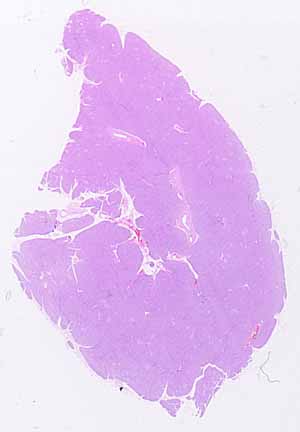
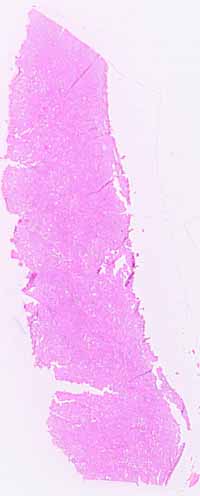
Slide ERG 19. Not many parts of the body are capable of yielding a tissue chunk of this size without including much internal texture visible to the unaided eye.
Here and there should be found patches of stromal tissue (collagen along with small blood vessels and ducts). In this specimen, the stroma is most conspicuous where it includes inflammatory infiltrate (lots of small lymphocyte nuclei).
The expanse of parenchymal tissue should be seen as mostly cuboidal cells, suggestive of glandular epithelium. But these epithelial cells do not form a typical epithelial surface. All together, such parenchyma interspersed with stromal patches containing blood vessels and ducts should suggest liver.
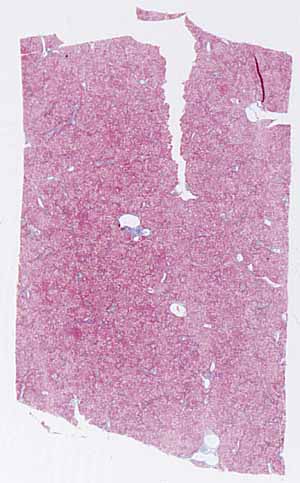
Slide ERG 20. As for the previous slide (ERG 19), not many parts of the body are capable of yielding a tissue chunk of this size without including much conspicuous internal texture visible to the unaided eye.
This specimen displays a trichrome stain, emphasizing collagen in small patches of stroma.
The hints page says that "this specimen is seriously pathological." Since I don't have access to the actual slides while preparing this page, I still need to look at the slide before describing the pathology here.
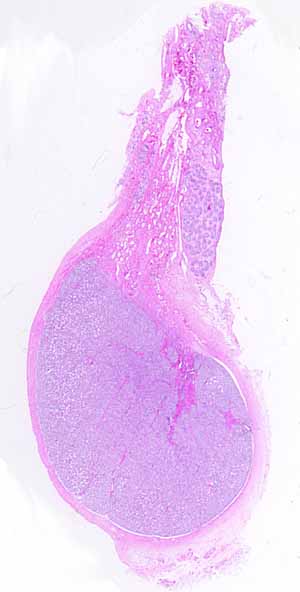
Slide ERG 21. This specimen is unusual enough that I'll just describe it here:
This is a testis from a pre-adolescent boy. It is lacking in the signs of spermatogenesis that characterize mature testes.
In addition to the mass of coiled seminiferous tubules that form the testis itself, this specimen includes rete testes, efferent ductules, epididymis, and mediastinum.
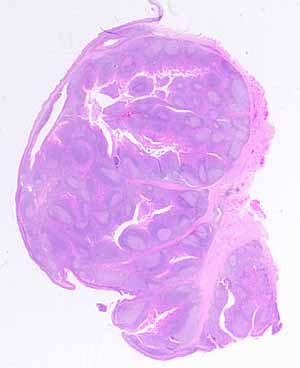
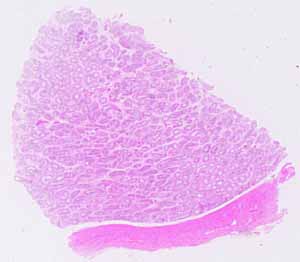
Slide ERG 22. The many tubules which comprise the parenchyma here, together with the thick collagen capsule, are characteristic of this organ. But most distinctive are the varied appearances of cell nuclei associated with the tubules, including especially those numerous, very tiny, very densely-basophilic specks -- the heads of spermatozoa.
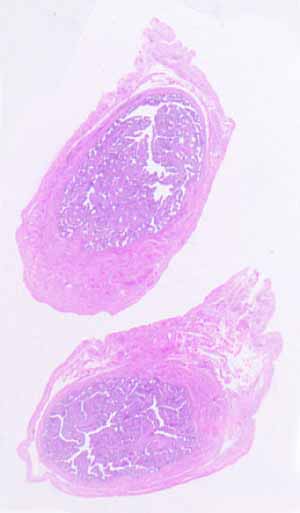
Slide ERG 23. This slide includes two sections of the same tubular organ. Note their actual size.
This tube has a thin muscular wall. Its lumen is almost entirely filled with mucosal tissue, much folded to leave only narrow channels between adjacent epithelial surfaces. Cilia should be visible on at least some epithelial cells. Such a configuration is typical of only one organ, the Fallopian tube.
Slide ERG 24. This slide carries sections from two similar pieces of the same organ.
Not much distinctive is noticeable at low magnification. With higher magnification, at first glance this specimen might look like a jumble of assorted cells with no apparent organization. Nevertheless (as with most specimens), there is no other organ quite like this one.
Peculiar glandular texture (i.e., clusters of cells that have an epithelial-cell appearance but which have no associated ducts), together with rich vasculature, should suggest endocrine tissue. That, as well as the organ's size and its thin capsule, should eliminate all endocrine glands except anterior pituitary.
For students: Introductory instructions for slide examination
Comments and questions: dgking@siu.edu
SIUC / School
of Medicine / Anatomy / David
King
https://histology.siu.edu/SAQcheat2.htm
Last updated: 28 December 2024 / dgk