Lower Tract:
Appendix, Colon, Rectum, and Anal Canal
The appendix, the colon, and the rectum all share a common mucosal description, with many straight crypts but no villi. The epithelium consists of many goblet cells interspersed among absorptive cells. The anal canal represents a transitional region, where the characteristics of the colon and rectal mucosa change to those of skin.
Layers of the lower tract
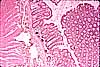
The mucosa of the colon has a simple columnar epithelium shaped into straight tubular crypts. There are no villi. The mucosa in appendix and rectum is similar to that of colon.
In cellular composition, the epithelium of the lower tract resembles that of the small intestine, but with a much higher proportion of goblet cells interspersed among the absorptive cells. (The proportion of goblet cells increases as one descends the tract, highest in the colon, higher in ileum than in jejunum and higher in jejunum than in duodenum.)
Goblet cells in the colon are so numerous and so large (bulging against the adjacent absorptive cells) that the colon epithelium sometimes appears to consist mostly of goblets. Nevertheless, as elsewhere along the intestinal tract, absorptive cells remain much more numerous than goblet cells.
The crypt epithelium also includes stem cells which replenish the epithelium every few days, enteroendocrine cells, and (in the cecum and proximal colon) Paneth cells.
The crypts are separated from one another by conspicuous lamina propria, whose composition is similar to that of small intestine: loose connective tissue infiltrated by many white blood cells, with capillaries and thin strands of smooth muscle.
Lymph nodules are a standard feature of the appendix but are normally relatively uncommon elsewhere in the lower tract.
More frequent accumulations of lymphoid tissue are characteristic of chronic inflammatory bowel disease. For more on inflammation of the colon, see Milikowski & Berman's Color Atlas of Basic Histopathology, pp. 258-265, or Robbins Pathologic Basis of Disease. Compare Crohn's disease, WebPath and ulcerative colitis, WebPath (low power), WebPath (high power).
The muscularis mucosa of the lower tract forms a thin layer (only a few muscle fibers in thickness) beneath the deep ends of the crypts.
The submucosa of the lower tract is relatively unspecialized.
Muscularis externa of the colon has the standard layers of inner circular and outer longitudinal smooth muscle, with ganglia of Auerbach's plexus scattered in between. The longitudinal muscle is gathered into three distinct bands, the taenia coli.
The outer layer of the colon is a serosa attached to mesentery.
Regions of the lower tract
Three regions of the lower tract -- the appendix, the colon, and the rectum -- have very similar tissue architecture. A fourth region, the anal canal, represents a transition where the characteristics of lower-tract mucosa change to those of skin.
The wall of the appendix follows the same layered plan as the colon, albeit with a much small diameter. The surface epithelium surface and the crypts are practically identical to those of colon.
However, the lamina propria of the appendix contains many lymph nodules and other, less organized lymphoid accumulations, so that it normally has an appearance which might suggest chronic inflammation if seen in the colon (or anywhere else).
In acute appendicitis, heavy leukocyte infiltration occurs throughout the wall of the organ. For images, see WebPath (gross), WebPath (low power), WebPath (medium power), and WebPath (high power), or Milikowski & Berman's Color Atlas of Basic Histopathology, pp. 274-275.
The colon proper is described above.
The colon is a common site for abnormal growths, such as adenomas and carcinomas. Colon biopsies, which reveal details of tissue arrangement and cellular appearance, provide material for determining whether or not a particular growth is malignant.
For images of benign adenomatous polyps (tubular adenoma), see WebPath (gross), WebPath (low power), WebPath (medium power). Compare these growths with villous polyps, WebPath (gross), WebPath (low power); with adenocarcinomas, WebPath (gross), WebPath (low power), WebPath (medium), WebPath (high power), WebPath (higher power); and with precancerous dysplasia, WebPath. Also see Milikowski & Berman's Color Atlas of Basic Histopathology, pp. 266-271.
The rectum has the same architecture as the colon, except for its location in the body wall rather than suspended in the peritoneal cavity. Thus its outer layer is adventitia rather than serosa.
The anal canal represents a transition from features of the lower tract to those of skin. The surface changes from a simple columnar epithelium with goblet cells, through a short zone of non-keratinized stratified squamous epithelium, to the keratinized stratified squamous epithelium that is typical of epidermis. Lamina propria and muscularis mucosae disappear distally, and the connective tissue of submucosa changes to the dense fibrous tissue of dermis. This connective tissue contains both ordinary eccrine sweat glands and much larger apocrine sweat glands. Smooth muscle of the colon changes to striated muscle of the voluntary anal sphincter.
Lower tract examples:
Comments and questions: dgking@siu.edu
SIUC / School
of Medicine / Anatomy / David
King
https://histology.siu.edu/erg/colon.htm
Last updated: 27 May 2022 / dgk