Histology Study Guide
Cardiovascular SystemThese notes are an ancillary resource, NOT a substitute for scheduled resource sessions or for textbooks. If you use this on-line study aid, please refer to your textbooks and atlases for richer, more detailed information.
- Blood (separate page)
- Blood vessels
- Composition
- Intima, endothelium
- Media, smooth muscle
- Adventitia, connective tissue
- Categories
- Lymphatic system
- Lymphatic vessels
- Lymph nodes and nodules
- MALT Mucosa-associated lymphoid tissue (e.g., tonsils)
- Spleen
- Thymus
SAQ -- Self Assessment Questions
SAQ, Cardiovascular and Lymphatic Systems
SAQ, Introduction -- microscopy, cells, basic tissue types, blood cells.
Blood vessels
Blood vessels are basically tubular organs found within other organs. (Recall that an "organ" consists of two or more different tissue types "organized" to serve a larger function.)
Larger blood vessels may even have smaller vessels within their walls (the vasa vasorum).
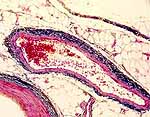
Histologically, blood vessels consist of concentric layers or "tunics" of different tissue types.
- The tunica intima is the inner lining, consisting of endothelium and a relatively thin layer of supporting connective tissue.
- The tunica media is the middle muscular and/or elastic layer, containing smooth muscle and elastic tissue in varying proportions.
- The tunica adventitia is the outer, fibrous connective tissue layer.
- Nervous tissue is generally inconspicuous in blood vessels but serves to regulate smooth muscle function and to mediate pain sensation.
Image © Blue Histology
Blood vessels are categorized by function. Different categories of vessels differ somewhat in the detailed composition of their layers.
- Note that arteries and veins tend to travel together, so histological sections often provide opportunities to compare an adjacent vein/artery pair.
- Arteries conduct blood away from the heart and have proportionately more smooth muscle and elastic tissue than veins of comparable size.
- Arteries are commonly sub-categorized into elastic arteries, muscular arteries, and arterioles.
- Veins return blood to the heart and have proportionately less smooth muscle and elastic tissue than arteries of comparable size.
Click on an image for enlargement.
- Capillaries and sinusoids communicate between arteries and veins. Their lining generally consists only of endothelium and underlying basement membrane.
Note that capillaries are found in connective tissue (or stroma) in nearly every organ (cartilage is an exception, an avascular connective tissue), but capillaries are seldom noticable in routine histological sections.
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Historical note: The tunica intima is also called Bichat's tunic," after Xavier Bichat (b. 1771), "the Father of Histology."The intima is the inner layer of a vessel. It consists of very thin lining of simple squamous endothelial cells supported by a similarly thin layer of connective tissue. The integrity of the intima is critical, since damage can lead to atherosclerosis or clotting.
- In arteries a continuous layer of elastic tissue, called the internal elastic lamina, forms the boundary between the intima and the media.
Endothelium
The endothelium is a specialized form of mesenchymally-derived epithelial tissue. This simple squamous epithelium forms a thin, delicate lining of all blood vessels as well as the heart and the lymphatic system. The endothelium is arguably the most significant feature of the vessel.
Capillary endothelium may have closely associated pericytes, cells with contractile properties which might regulate capillary flow.
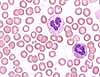
Endothelial cytoplasm is inconspicuous in routine light microscopy. Typically only the nuclei are noticeable, at the boundary between the lumen and the wall of a vessel.
In cross section, endothelial nuclei typically appear thin and dark. However, occasionally endothelium lies parallel to the plane of section. In this case the nuclei may appear very large, round, and pale.
Although endothelial cells appear rather uninteresting under the microscope, these are important cells. They are situated at a critical location, between the blood and all other body cells. They secrete substances which control local blood flow and blood coagulation, and they are active participants in white blood cell emigration during inflammation.
Historical note: The close association of endothelium with macrophages in liver, spleen and lymph nodes (i.e., those organs with elaborate endothelially-lined channels supported by reticular connective tissue) led to the term reticuloendothelial system. The name reflects former confusion about the distinction between endothelial cells and the scattered population of macrophages (monocytes, histiocytes). Macrophages can be readily labelled through their phagocytosis of experimentally-injected carbon particles. However, endothelial cells are also labelled by the same procedure. Although endothelial cells are not dramatically phagocytotic, they do shuttle some materials across the endothelial lining via small endocytotic and exocytotic vesicles.
Continuous endothelium. Throughout much of the body, the capillary endothelial lining is continuous, with neither large gaps between cells nor holes through cells. Materials pass across the endothelium either by diffusion or via rapid vesicular transcytosis. (In most of the brain, a lack of transcytotic vesicles accounts for the blood brain barrier -- the only substances which cross such a barrier are those which can diffuse through plasma membranes or those for which specific membrane channels exist.)
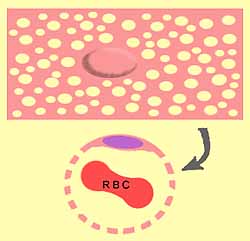
Fenestrated endothelium. In a few special locations -- notably in the sinusoids of the liver, in the glomeruli of the kidney, and in most endocrine glands -- the endothelium is fenestrated (i.e., full of holes -- from fenestra, window; see cartoon image at right).
Consult your histology textbook and/or atlas for additional detail and electron micrographs of endothelial cells.
- Variations in the endothelial lining determine how freely blood components can leave the vessel (see capillaries).
- Perhaps even more critically (at least from a clinical perspective), the endothelium must allow blood to flow freely past without any disturbance that might trigger clotting. And yet, the endothelium must also be ready to alter its membrane properties to allow white blood cells to adhere and emigrate in response to inflammation.
Atherosclerosis and blood clots may develop when the intimal lining of a vessel is damaged.
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
The media is the middle layer of a blood vessel. In most arteries and veins it is the thickest of the three tunics.
- The thickness of the media is generally proportional to the overall diameter of the vessel.
The media consists of smooth muscle and elastic tissue in proportions which vary according to the type and size of vessel. Elastic arteries have the highest proportion of elastic tissue while muscular arteries have the highest proportion of smooth muscle.
- In arteries a continuous layer of elastic tissue, called the internal elastic lamina, marks the boundary between the media and the intima.
- In most vessels, the smooth muscle fibers are arranged circumferentially, so the plane of section across a vessel can be deduced by the orientation/shape of smooth muscle nuclei.
Elongated smooth muscle nuclei indicate longitudinally-cut muscle fibers and hence a transversely-sectioned vessel.
- Tiny round smooth muscle nuclei indicate transversely-cut muscle fibers and hence a longitudinally-sectioned vessel.
- (Curiously, veins in the adrenal medulla have bundles of smooth muscle arranged longitudinally.)
TOP
OF THIS PAGE / CONTENTS
FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Ordinary fibrous connective tissue
forms the outer, adventitial layer of blood vessels, as it does for most tubular organs. This adventitial connective
tissue is usually more or less continuous with the stromal connective tissue
of the organ in which the vessel is found. That is, there is not a distinct
outer boundary to the tunica adventitia. Nevertheless, the fibers of adventitial connective tissue tend to be more
concentric around the vessel and often somewhat denser than the surrounding
connective tissue (fascia). Tunica adventitia may also contain numerous elastin
fibers. Clinical note: The presence of adventitial connective tissue
tightly adhering to vessels facilitates the surgical isolation and repair
of vessels.
TOP OF THIS PAGE / CONTENTS
FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Arteries The largest arteries, such as the aorta and its larger branches, have a tunica
media dominated by elastic tissue.
The elasticity conferred by elastin allows these elastic arteries to
smooth out the sharp changes in blood pressure resulting from the pumping
heart. Most arteries are muscular arteries, with a
media dominated by smooth muscle. But
elastin is also a substantial component. Arterioles Arterioles are
the smallest arteries. Note that gross anatomists and surgeons
may use the term arteriole for any very small artery. Histologists
tend to use the term only for terminal arterial vessels
(i.e., those immediately preceding a capillary bed). Terminal (histological) arterioles are characterized
by having only a single layer of smooth
muscle cells.
Because smooth muscle fibers
are arranged circumferentially, the plane of section across an arteriole
can be inferred by the orientation/shape of smooth muscle nuclei.
Most arteries have a continuous layer of elastin, called the internal elastic
lamina, at the boundary between the media and the
intima. The thickness of arterial walls is typically not much less than the diameter
of the lumen. With such relatively thick walls, arteries tend to retain
a round cross-section in postmortem histological preparations (in contrast
to veins, which tend to appear more flattened). Note that arteries of pulmonary
circulation (which convey blood of lower pressure than systemic circulation)
have relatively thinner walls, similar to systemic veins. TOP OF
THIS PAGE / CONTENTS
FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Veins Veins have a wall similar to that of arteries
but with a thinner tunica media. The thickness of vein walls is typically much less than the diameter of the
lumen (i.e., proportionately much thinner than arteries carrying a similar
volume). With such relatively thin walls, veins tend to appear flattened
or collapsed in cross-section in postmortem histological preparations
(in contrast to arteries, which tend to appear more
round). Note that vessels of pulmonary
circulation (which convey blood of lower pressure than systemic circulation)
have relatively thinner walls than systemic vessels of comparable diameter. TOP
OF THIS PAGE / CONTENTS
FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Capillaries and sinusoids Capillaries and sinusoids are the smallest (microscopic) vessels, providing
communication between arteries
and veins. Historical note: The existence of capillaries
was predicted by William
Harvey in 1628, as a necessary corollary of his theory of blood circulation.
Capillaries were actually observed in 1661 by Marcello
Malpighi using a newly invented instrument, the microscope. For a more thorough account of historical understanding of capillaries, see
"The history of the capillary wall:
doctors, discoveries, and debates," by C. Hwa and W.C. Aird, in
Am J Physiol Heart Circ Physiol 293: H2667-H2679 (2007),
doi:10.1152/ajpheart.00704. NOTE: In histological preparations, capillaries tend to be quite inconspicuous
unless they contain red blood cells. Capillary endothelial nuclei are seldom close together and
are commonly difficult to distinguish from fibroblasts and other connective
tissue cells, unless the preparation is fine enough to resolve the thin
endothelial cytoplasm surrounding a small lumen.
Adventitia
(tunica adventitia)
Examples of typical muscular arteries.
Click on an image for enlargement and comparison with an adjacent vein.




Click on
a thumbnail below to enlarge an image.
Each image includes a small artery or arteriole.

Also see EM images of blood vessels,
from Electron Microscopic Atlas of cells, tissues and organs in the internet).
In
routine histological sections, the internal elastic lamina of transversely-sectioned
arteries typically displays a distinctive sinusoidal appearance, resulting
from postmortem contraction of the artery's smooth muscle in the absence
of normal blood pressure.
Historical note: William
Harvey first recognized the function of valves in veins, which he described in his
de Motu Cordis, 1628. Harvey also described how these valves could be demonstrated
in an everyday classroom setting (see here).
Examples of typical veins.
Click on an image for enlargement and comparison with an adjacent artery.


Historical note: Ignoring
inconspicuous tissue features such as capillaries can have consequences. Since stromal capillaries
are seldom evident in tissue specimens, they are often ignored and forgotten. Unfortunately,
just such inattention may have delayed for decades the realization that
interfering with tumor vasculature might powerfully inhibit tumor growth.



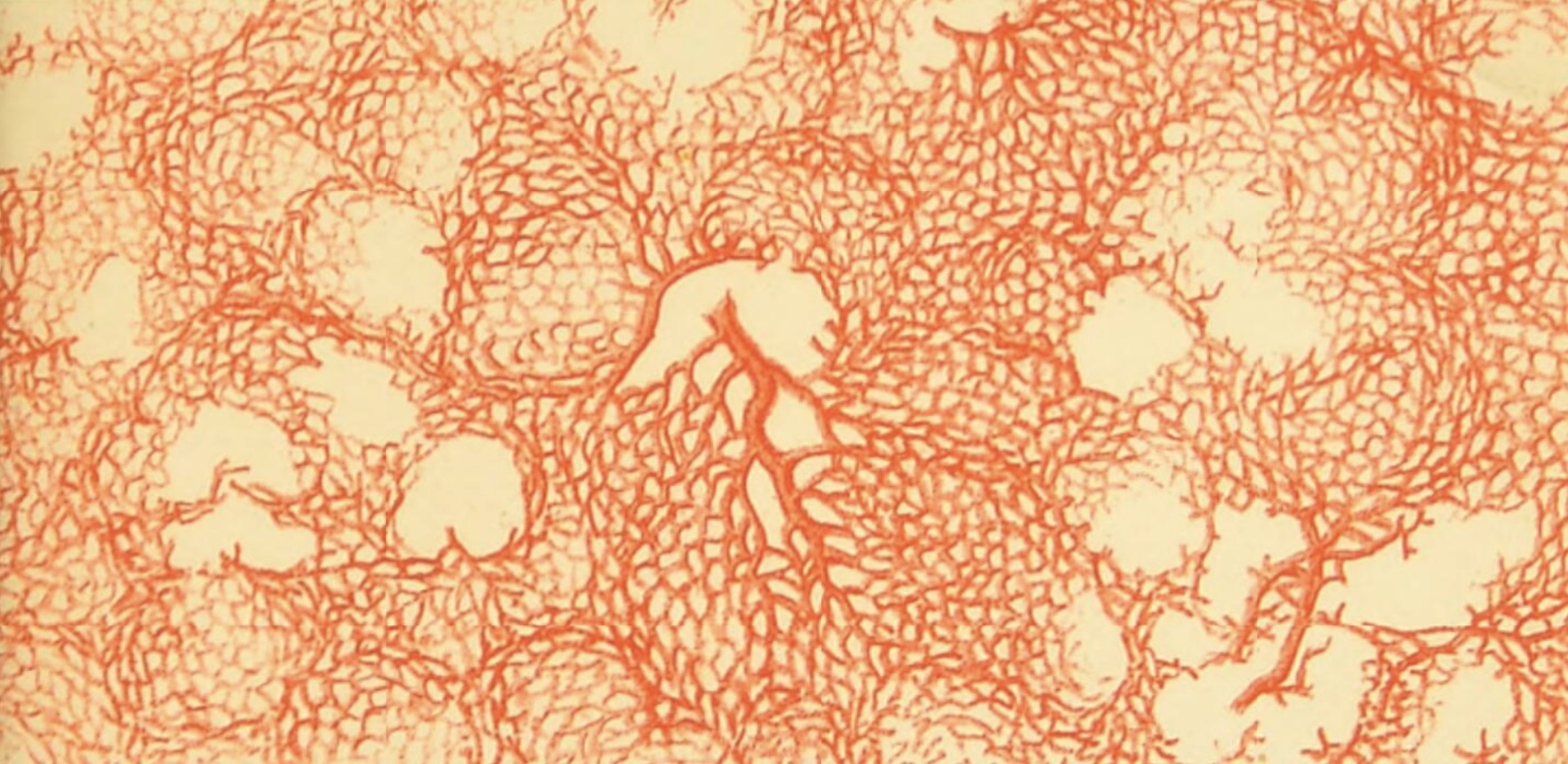
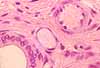
By definition, capillaries are vessels whose diameter is so small (less than 10µm) that red blood cells must pass through in single file (thumbnail at left).
Capillaries often form an interconnected plexus, or "capillary bed." Thumbnails at right show capillaries within lung, kidney and stomach.
In contrast to capillaries, sinusoids are typically more voluminous (for an example, see liver). Although the lumen of a sinusoid is commonly narrow in one dimension, it may be extensive in another dimension, like an alley-way space between the walls of adjacent buildings rather than the hollow of a tube.
The
walls of capillaries and sinusoids consist of little more than endothelium.
A single thin, flattened endothelial cell forms a segment of capillary, like
a sheet of paper rolled into a tube (with a small bulge at the site of the
nucleus). These single-cell tubes are then attached end-to-end to form
a capillary.
Wrapped at intervals around capillaries are pericytes (originally called Rouget cells, after C.M.B. Rouget, b. 1824), cells with contractile properties that can apparently adjust capillary blood flow. This effect has been demonstrated for local microvascular control of blood flow in the brain.
Research notes:
MacVicar & Salter, Neuroscience: Controlled capillaries, Nature 443, 642-643 (12 October 2006) | doi.org/10.1038/443642a. Dore-Duffy & Cleary, Morphology and properties of pericytes, Methods in Molecular Biology, vol. 686, pp. 49-68 (2011) | doi.org/10.1007/978-1-60761-938-3_2. Sweeney, Ayyadurai & Zlokovic, Pericytes of the neurovascular unit: key functions and signaling pathways. Nature Neuroscience 19, 771-783 (2016) | doi.org/10.1038/nn.4288.
In most parts of the body, capillaries and sinusoids are more or less "leaky." The degree of "leakiness" is determined by variations in the endothelial lining of the capillaries.
In ordinary connective tissue, plasma leakage is typically balanced by re-absorption and/or lymph drainage. A shift in the balance (e.g., increased vascular permeability due to inflammation) can result in accumulation of tissue fluid, or edema.
|
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Heart
The lining of the heart is similar to that of blood vessels, with an intima including endothelium.
The pericardium (the heart's outer surface) is a serosa lined by mesothelium.
Mesothelium -- a simple squamous epithelial tissue, derived from mesoderm -- forms the surface lining not only the pericardial cavity but also peritoneal and pleural cavities (i.e., all major body cavities).
The bulk of the heart consists of cardiac muscle, one of the three distinct types of muscle in the body. (The other two muscle types are skeletal muscle and smooth muscle.)
Cardiac pathology yields characteristic changes in the structure/appearance of cardiac muscle.
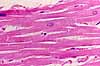
Cardiac muscle has several distinct characteristics.
- Cardiac muscle is striated, like skeletal muscle. (For brief description of striations, see skeletal muscle.)
- Cardiac muscle consists of distinct, individual cells (unlike skeletal muscle which consists of immensely long, multinucleate fibers).
- Cardiac muscle cells are attached end-to-end by specialized junctions called intercalated discs.
Intercalated discs consist of adhering junctions (into which the contractile myofilaments are attached) and gap junctions (which allow passage of ions thereby establishing electrical connection between adjacent cells.)
For detailed images of intercalated discs, see the Electron Microscopic Atlas of cells, tissues and organs in the internet:
- Each end of a cardiac muscle cell may attach to two or more other cells, so that the fibrous structure of cardiac muscle appears to be branched (unlike skeletal muscle, where each fiber is a single, discrete unit).
For more information about cardiac muscle cells, see your textbook.
For more electron micrographs of heart muscle, see the Electron Microscopic Atlas of cells, tissues and organs in the internet.
Specialized cardiac muscle cells form bands called Purkinje fibers (named after Johann Purkinje, b. 1787), which conduct electrical signals to coordinate heart contractions (see your physiology resources). Purkinje fibers have a larger diameter and paler cytoplasm (i.e., fewer contractile filaments) than ordinary cardiac muscle fibers. Both of these features are adaptations for reducing electrical resistance and increasing the speed of electrical conduction.
See WebPath Myocardial Infarction for description and images of cardiac pathology.
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Lymphatic System
The lymphatic system consists of:
- lymphocytes -- characteristic cells of the immune system;
- lymph vessels -- channels which eventually drain into the thoracic duct and hence into the vena cava;
- lymph nodes -- specialized organs along lymph vessels, where lymphocytes proliferate;
- mucosa-associated lymphoid tissue -- like lymph nodes, sites where lymphocytes proliferate;
- spleen -- another site where lymphocytes proliferate, and where worn-out red blood cells are recycled;
- thymus (and bone marrow) -- organs where lymphocytes originate.
Key for microscopic differentiation of lymphoid tissues (courtesy M. O'Keefe, MSI)
The lymphatic system serves two principal functions.
- The lymphatic system provides a route for excess interstitial fluid ("lymph") to return to the blood.
- The lymphatic system provides the means for immune system cells (most notably lymphocytes) to travel, communicate, and proliferate; thus the lymphatic system is instrumental in the process of immunological defense, including inflammation.
(Continue down this page for additional introductory material. However, an in-depth treatment of the immune system is beyond the scope of this website.)
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Lymphatic vessels
Lymphatic vessels (often just called lymphatics) are channels which drain excess fluid ("lymph") from tissues.
In most peripheral tissues, some plasma seeps out of capillaries. A portion of this is taken back up in venules while the rest drains into terminal lymphatic channels, also called lymphatic capillaries. A shift in the balance between fluid entering and leaving tissues (e.g., increased vascular permeability due to inflammation) can result in accumulation of tissue fluid, or edema.
All lymphatic vessels eventually lead "downstream" to the thoracic duct, which empties into the vena cava (a point where blood pressure is quite low; higher pressure would impede drainage).
Directional flow in lymphatic vessels is maintained by Swammerdam valves (commemorating Jan Swammerdam, b. 1637).
Lymphatic vessels resemble blood vessels with exceptionally delicate walls (and, of course, without red blood cells). Smaller lymphatic vessels consist of little more than endothelium.
If, while examining a histological specimen, you encounter a flattened, endothelially-lined passage that seems too delicate to be a vein but too large to be a capillary, it is probably a lymphatic.
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Lymph nodes and nodules

Lymph nodes are small organs, found in scattered locations along the lymphatic drainage system of the body.
Some lymph nodes can be palpated, where they are sometimes called "glands," especially when swollen in reaction to infection.
Lymph nodes provide "gathering places" through which wandering lymphocytes must pass as they travel from peripheral tissues on their return to systemic circulation. Within the lymph nodes, activated lymphocytes (i.e., those which have encountered an antigen which they recognize) proliferate, producing more lymphocytes able to respond to the same antigen.
Metaphorically, lymph nodes might be considered to be "filters" for peripheral interstitial fluid.
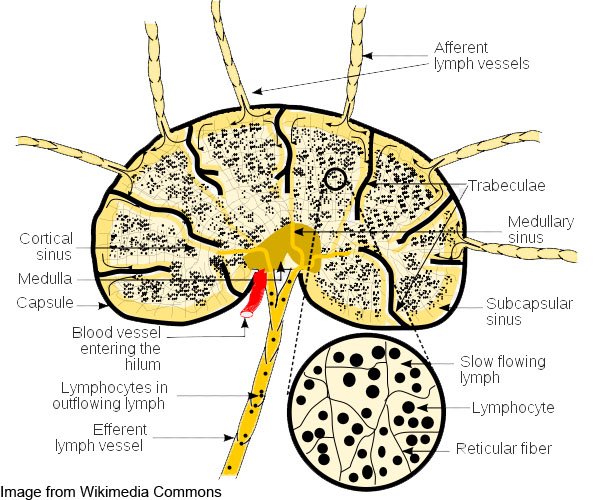
Lymph nodules cluster toward the cortex of the lymph node, where afferent lymph vessels pass through the capsule. The medulla appears less visibly organized. An efferent lymph vessel drains the lymph node from the hilus, in the region of the medulla (diagram). A lymph node also receives circulating blood coming in through the hilus and passing through "high endothelial venules, specialized for interacting with the lymphocytes.
Lymph nodes consist of a fibrous connective tissue capsule enveloping many lymphocytes and other immune-system cells, into and through which lymph flows (diagram). The parenchyma of a lymph node is organized into cortex and medulla. In the cortex, lymphocytes are gathered into lymph nodules, also called lymphoid follicles, which are sites where lymphocytes congregate. At the center of each lymph nodule is a germinal center where lymphocytes proliferate.
Lymph nodes are supported within by a network of reticular fibers.
For additional information, see your text.
Key for microscopic differentiation of lymphoid tissues (courtesy M. O'Keefe, MSI)
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Mucosa-associated lymphoid tissue ("MALT") and Gut-associated lymphoid tissue ("GALT")
Lymphoid tissue occurs in lamina propria of most mucosal organs, where it is sometimes referred to as MALT (Mucosa-Associated Lymphoid Tissue), most conspicuously in the gastrointestinal tract, where it is sometimes referred to as GALT (Gut-Associated Lymphoid Tissue).
The most characteristic features of mucosa-associated lymphoid tissue are lymph nodules, also called lymphoid follicles, which are sites where lymphocytes congregate. At the center of each lymph nodule is a germinal center where the lymphocytes proliferate.
The connective tissue around a lymph nodule is usually heavily infiltrated with lymphocytes migrating to and from the germinal center.
Lymph nodules may occur in lamina propria anywhere along the GI tract. Large aggregations of lymph nodules may extend beyond lamina propria and intrude into the submucosa. Nearby epithelial tissue may also be infiltrated by lymphocytes.

Aggregations of lymph nodules are characteristic of tonsils, Peyer's patches, and appendix.
For more on MALT, consult your histology text.
Key for microscopic differentiation of lymphoid tissues (courtesy M. O'Keefe, MSI)
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Spleen

The spleen is an organ in which lymphoid tissue and blood are intermixed and served by a network of vascular sinusoids. The loose lymphoid and blood cells are contained within a fibrous connective tissue capsule and supported by strands of fibrous connective tissue ("trabeculae"). Lymphoid tissue forms the so-called "white pulp" while surrounding tissue rich in blood forms "red pulp."
The spleen is enclosed by a tough capsule of dense collagenous connective tissue. Arteries enter the capsule, extend some distance into the body of the spleen where they tend to be surrounded by white pulp, and then open into sinusoids in the capsular space. So, circulation within the spleen is essentially open, unconstrained by capillaries or veins. Leaving the spleen, a portal vein carries blood to the liver.
The color names for red and white pulp reflect their natural (unstained) color, with red pulp colored by red blood cells while white pulp takes on the creamy color of massed lymphocytes (similar to pus).
For more detailed description of spleen structure and function, consult your text.
Key for microscopic differentiation of lymphoid tissues (courtesy M. O'Keefe, MSI)
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.
Thymus
The thymus is the primary organ for maturation of lymphocytes. It plays a central role in developing self-tolerance (i.e., the immune system's ability to avoid attacking the body's own cells). "Promiscuous gene expression" in stromal epithelial cells of the thymus leads to deletion of T-cells that react to self-antigen. (A similar process has been detected in peripheral lymph nodes; see Science 321:776, 8 August 2008.)

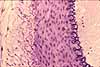
Superficially, the thymus resembles a gland subdivided into numerous small lobules. But the thymus has no ducts and no proper secretory tissue. In an active (i.e., young) thymus, the cortex of each lobule is densely packed with lymphocytes while each lobule has a paler medullary core where cells are dividing. The thymus also contains cells called "reticular cells," "epitheliocytes," "dendritic cells," and "stromal cells." Although such cells are generally inconspicuous in routine histological specimens, clusters may be evident as "Hassall's corpuscles" (commemorating Arthur Hassall, b. 1817).
Research news: Hassall's corpuscles have been associated with the processes of T cell selection. See, e.g., Nature 436: 1181-1185; (2005).For more information on thymus structure and function, consult your text.
Key for microscopic differentiation of lymphoid tissues (courtesy M. O'Keefe, MSI)
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE / CARDIOVASCULAR IMAGE INDEX.


Cardiovascular pathology
WebPath offers an extensive image collection for blood and bone marrow smears, both normal and pathological.
WebPath also provides a tutorial on myocardial infarction and an extensive set of images associated with atherosclerosis. Note especially the following specific examples
- Pulmonary thromboembolus (animated diagram).
- Pulmonary embolus.
- Structure of a thrombus.
- Occlusive coronary atherosclerosis.
- Atherosclerotic narrowing of coronary artery, contrast with normal coronary artery.
- Coronary thrombosis.
- Atheromatous plaque, low power / high power.
- Myocardial infarct after 1-2 days / after 3-4 days / after 1-2 weeks, contrast with normal myocardium.
- Dissecting aorta / higher magnification.
- Renal hyperplastic arteriosclerosis.
- Renal hyaline arteriosclerosis with glomerulosclerosis.
- Calcific sclerosis (nice to compare with above pathologies).
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE
Image index
TOP OF THIS PAGE / CONTENTS FOR THIS PAGE
 Comments
and questions: dgking@siu.edu
Comments
and questions: dgking@siu.edu
SIUC / School
of Medicine / Anatomy / David
King
https://histology.siu.edu/crr/cvguide.htm
Last updated: 10 May 2025 / dgk